Asking for ‘Consanguinity’ in a couple ? – Rather ask for ‘Endogamity’
Nov 22, 2016
43821 Views
As an experienced Ob/Gyn/ Infertility doctor, when a couple comes to you for their preconception visit or confirmation of an early pregnancy, you may be asking for certain ‘significant’ family history or whether the husband and wife are ‘related by blood’ (first-cousins/ ‘mene rikam’ or uncle-niece/ ‘mene maama – mene kodalu’ as they say it here in Andhra and Telangana states).
Sitting in my Genetic Clinic at Mapmygenome, when I am looking at a non-consanguineous healthy couple whose child has a severe genetic disorder, I wonder why the family history does not mention that they belonged to the same community or caste, even if there was no ‘direct blood relation’? But, as soon as I asked this to myself, I realized why. Endogamous marriages (within the same caste or community) are embedded in the Indian cultural practice, – and is so common, that it is often not considered ‘significant’ family history that may have implications for the next generation, especially in the presence of a genetic condition in the family.
In India, the genetic risks in children of ‘consanguineous’ couples and ‘endogamous’ couples is almost similar due to the traditional and continuing practices of marrying within the same caste and/ or community. This has resulted in the concentration of gene pool in small communities. Infact, certain genetic diseases are prevalent exclusively in the Indian sub-continent.
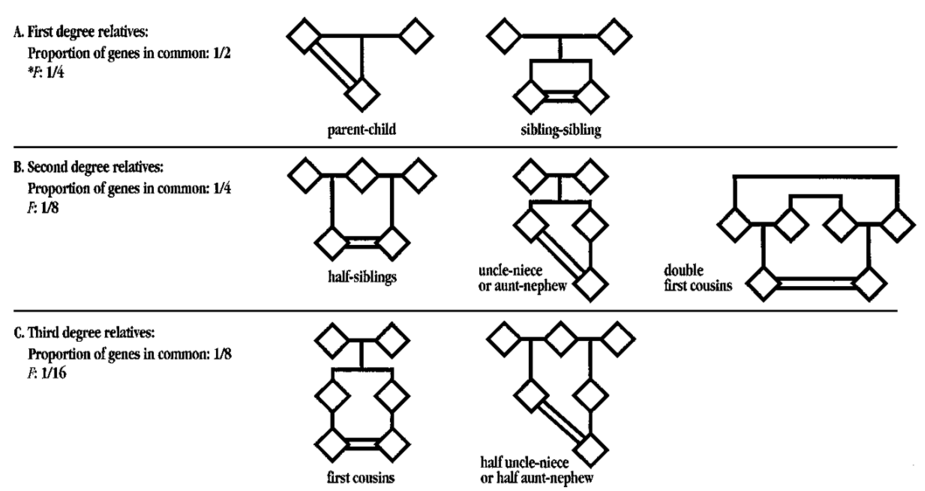
Figure 1: Pedigree of common consanguineous relationships: For example, an uncle and niece are predicted to share 25 % (1/4) of their genes, thus on average their children will be homozygous at 12.5% of gene loci. Similarly, first cousins would share 12.5% of their genes, hence their children would be homozygous at 6.25% of gene loci (Adapted from Bennett et al, 2002).
As a clinician, if you do see a couple, either consanguineous or endogamous, then what do you do next?
– Do you just make a note of it in the patient’s consultation sheet, and leave it at that? Or do you explain the associated risks to the fetus and how they can be screened for it? Or, do you refer the couple to a Genetic Counselor for pedigree analysis and recommendations?
Some of you may feel – ‘If we can’t do anything about the increased risk of birth defects and genetic disorders, let’s not worry the couple unnecessarily?’ Other may think ‘Is there really a serious risk to fetus, that warrants any action at all?’. And a lot of you could be pressed for time, considering your busy clinic hours and may not have the patience or enough information to answer the several queries from the couple that will follow as soon as you tell them that there is a genetic risk to the fetus due to the parental relatedness.
Your concerns are valid. This executive summary aims to clarify just these apprehensions! Nothing more, nothing less.
Yes, the risk of genetic diseases (leading to severe physical and/or intellectual disability), structural birth defects and congenital major malformations are almost 2 to 4 folds higher in children of ‘related’ / close endogamous couples (see Table 1). Most of the common genetic diseases seen in a higher frequency in children of ‘related’ parents are autosomal recessive conditions (that arise due to inheritance of two copies of the defective genes, one from each parent). Examples of these would be thalassemia, sickle cell anemia, spinal muscular atrophy, congenital sensorineural hearing loss, blindness and more than 100 metabolic diseases such as phenylketonuria, Galactosemia, Gaucher disease, methylmalonic academia, Friedreich ataxia. As a geneticist, we know that most of the rarest genetic diseases are tend to be found in children born out of consanguineous unions.
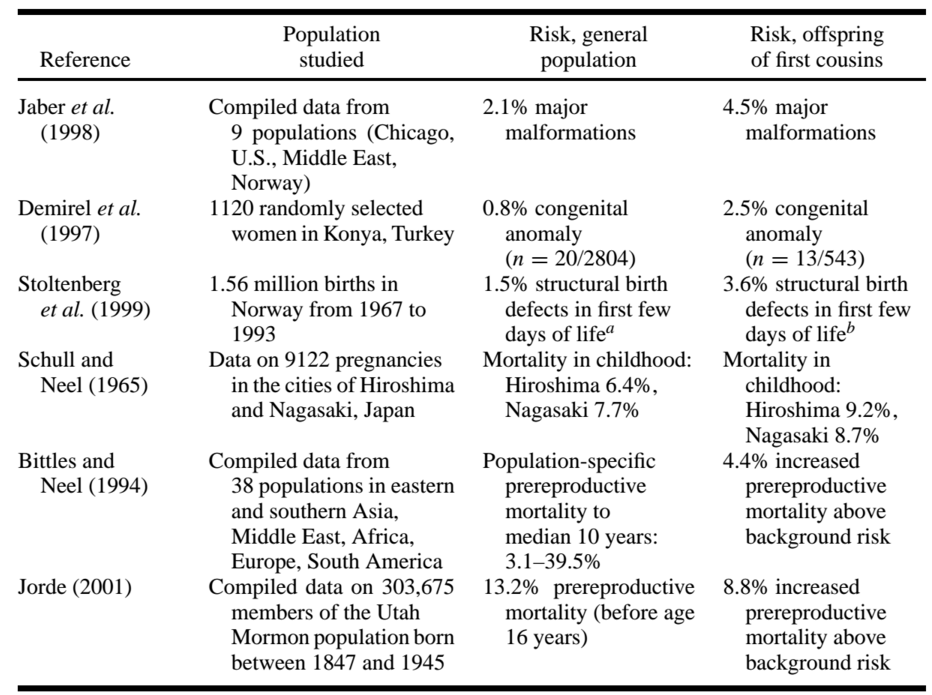
Table 1: Compilation of risks in children of ‘related’ couples, as compared to the baseline risk in general population (Adapted from Bennett et al, 2002).
The reason why Genetic Clinics are focusing on prevention of these diseases is because most of them do not have a cure as yet. If a child is born with any of the above conditions, there can be significant physical and/or mental disability for which treatments are only symptomatic and rarely curative. Both the quality of life of the child and parents is majorly affected. For a few metabolic diseases, there is some dietary modifications that can be made to reduce the associated morbidities, if diagnosed and treated very early.
Most of the couples benefit greatly from a prenatal/ preconception genetic counseling where they are educated about the implications of the couple’s relatedness, three-generation family history is studied, red flags such as newborn deaths, still births, developmental delay, physical or mental disability in family members are properly documented and analysed for overall risk assessment, risks to fetus/ future child is explained and most importantly, prognosis of the disease, it’s available treatment and options for prevention are discussed.
The more closer the community or relationship, the higher is the shared proportion of genes between the couple, and and consequently a much higher probability of both being asymptomatic carriers of the same genetic condition. While such carrier couples themselves may not be affected, can potentially pass on the defective genes to their child leading to a serious disease (1 in 4 chance of that happening). This may be predicted preconceptionally if the couple get themselves screened for carrier status of the common genetic diseases (Preconception couple carrier testing).

No, this test is nothing like the chromosomal karyotyping ordered routinely for couples with recurrent abortions/ bad obstetric history (BOH). This molecular (DNA based) genetic test is based on cutting edge next-gen-sequencing (NGS) technology and is highly sensitive for detecting carrier status of the couple in more than 170 to 300 disease genes. The post-test genetic counseling session with a senior Board-Certified Genetic Counselor ensures appropriate understanding of test results and a discussion of testing options during pregnancy.
In the scenario where both partners are found to be carriers of a disease, they are counselled of the prognosis of the disease and the available treatment options. If the couple are keen to prevent such disease, invasive prenatal diagnosis (amniocentesis/ chorionic villi biopsy) involving direct fetal genetic testing may be offered between 12 to 16 weeks gestation. The couple is also told about the other options such as using assisted reproductive technique (ART) with a donor gamete (to reduce risk – however, carrier testing in donor becomes important), or using preimplantation genetic diagnosis (to screen and select genetically healthy embryos for implantation).
Apart from the early genetic counseling referral and carrier testing of couple, other routine prenatal screening tests such as the first trimester dual/ triple marker screen (with NT scan), non-invasive prenatal testing (NIPT – for highly sensitive chromosomal risks in fetus) and serial detailed fetal anomaly scans are also highly recommended. Postnatal recommendations include newborn testing for metabolic defects by both biochemical (newborn screening done with dried blood spots at 2-7 days of birth) and molecular methods (BabyMap – diagnostic and confirmatory value).
For any assistance, queries, referrals for Certified Genetic Counselors and genetic testing requirements, feel free to contact MapMyGenome. Address: Mapmygenome India Ltd., Royal Demeure, HUDA Techno Enclave, Plot No.12/2, Sector-1, Madhapur, Hyderabad-500 081, India. Contact: 18001024595. Email: info@mapmygenome.in
About Mapmygenome
Mapmygenome is a molecular diagnostic and genetic counseling Centre with a technical expertise of 15+ years in the domains of genomics and molecular genetics big data analysis. We provide a one-stop solution for all genetic services to clinicians. Our teams at Hyderabad, Mumbai, Goa & Delhi comprise of biotechnologists, statisticians, Senior board-certified genetic counselors, scientists, bioinformaticians, and medical counselors. Our advisory panel has expert scientists and doctors of different medical disciplines. In order to enhance this innovative brand and to provide value-added services to clinicians and their patients, our highly-skilled research team works on cutting-edge technologies in various domains.

